
ANCA-associated vasculitis overview
 Fact-checked by
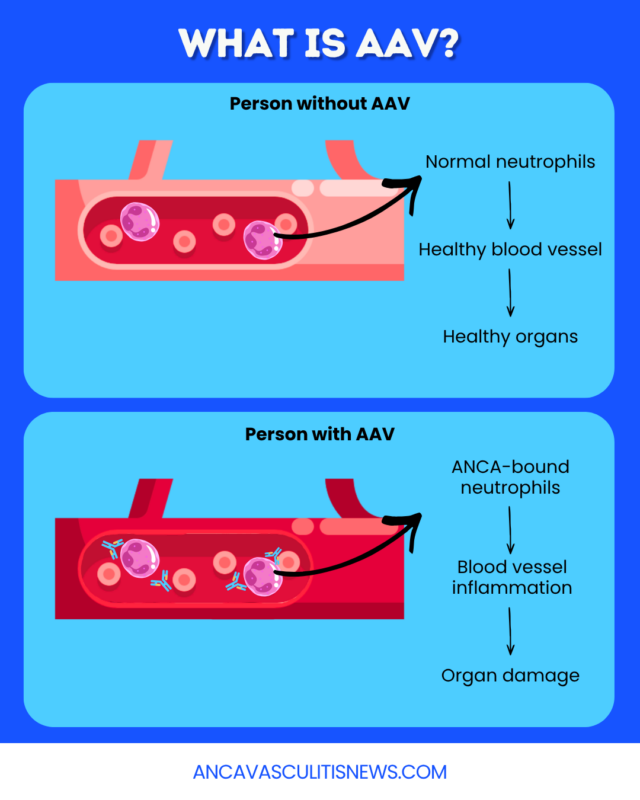
Fact-checked by ANCA-associated vasculitis (AAV), also called ANCA vasculitis, is a group of autoimmune diseases characterized by inflammation and damage of small blood vessels.
Typically, anti-neutrophil cytoplasmic antibodies, or ANCAs, drive these autoimmune attacks, which can occur throughout the body. AAV symptoms vary depending on which organs and tissues sustain damage, but commonly include problems in the kidneys, lungs, and upper airways.
AAV is a relatively rare condition, estimated to affect around 200 people per million globally. There is no cure for the disease, but with early diagnosis and modern immunosuppressive treatments, AAV prognosis has been steadily improving.
Causes
AAV is caused by the immune system’s mistaken attacks on small blood vessels. In most cases, self-reactive ANCAs are the drivers of these autoimmune attacks.
ANCAs typically recognize and bind to one of two proteins — myeloperoxidase (MPO) or proteinase 3 (PR3) — on immune cells called neutrophils. This activates the neutrophils, which then lead an assault on the cells lining small blood vessels, causing inflammation and damage.
Researchers don’t know exactly what triggers AAV autoimmunity, but genetic and environmental factors likely contribute. For genetically susceptible individuals, external factors that can contribute to AAV disease activity include:
- air pollution
- silica dust from sand, soil, and rock
- bacterial, viral, and fungal infections
- certain medications
- vaccines (rarely)
A minority of people with AAV do not have detectable ANCAs. Scientists are working to understand how AAV develops in these individuals.
Types of AAV
The three main AAV types are:
- microscopic polyangiitis (MPA)
- granulomatosis with polyangiitis (GPA)
- eosinophilic granulomatosis with polyangiitis (EGPA)
MPA most often affects the kidneys, lungs, skin, and nerves. Unlike the other types of AAV, granulomas, or masses of immune cells, don’t form at the site of inflammation. MPA is most often associated with MPO-ANCAs.
GPA typically damages the lungs, kidneys, and upper respiratory tract, with granulomas forming in these areas or other affected organs. GPA is most often associated with PR3-ANCAs.
EGPA is the least common type of AAV and often affects the lungs and upper respiratory system. Granulomas, primarily formed from white blood cells called eosinophils, drive this damage. Many people with EGPA do not have detectable ANCAs.
Any AAV type can have severe or life-threatening consequences, depending on the specific antibody type and pattern of organ involvement.
Common symptoms
AAV symptoms vary depending on where inflammation and damage occur, but may affect:
- ears, nose, and throat or sinuses (air-filled spaces in the skull)
- lungs
- kidneys
- skin
- nerves
- eyes
- gastrointestinal tract
Ear, nose, and throat, and sinus symptoms of AAV can include pain and congestion in the ears or upper respiratory system. AAV lung symptoms may include coughing, wheezing, and difficulty breathing.
AAV kidney involvement can progress quickly if untreated. Symptoms may include bloody or foamy urine and urinating less than normal.
Purplish patches or bluish-purple mottling, reflecting bleeding under the skin, are among the common AAV skin symptoms, while nerve damage in AAV can cause symptoms such as tingling, numbness, or muscle weakness.
Some patients also experience nonspecific constitutional symptoms that are not linked to a specific organ and can resemble signs of other autoimmune and inflammatory conditions. These may include:
- fever
- weight loss
- fatigue
- muscle or joint pain
Diagnosis
The wide range of possible AAV symptoms can make the disease challenging to recognize. Reaching an AAV diagnosis may involve several tests, including:
- a physical exam and review of symptom history
- blood and urine tests
- imaging
- microscopic examination of tissue samples, or biopsies
ANCA blood tests can detect ANCAs but can’t confirm or exclude AAV in isolation. Other blood and urine tests may reveal signs of systemic inflammation or specific organ damage.
Imaging tests, including CT scans and X-rays, can help visualize inflammation and damage in specific organs. Biopsies can reveal microscopic signs of AAV-related inflammation in tissues such as the kidneys, nerves, skin, or lungs.
To confirm the diagnosis, physicians also need to exclude other conditions with similar symptoms, including infections and other autoimmune diseases.
Treatment and management
AAV treatment typically occurs in two phases:
- induction: aims to quickly control immune attacks and drive the disease into remission, where symptoms are eased or absent
- maintenance: aims to sustain remission and prevent relapse
Both phases involve immunosuppressant medications, and the specific treatment regimen depends on several factors, including the treatment phase, disease type, and symptom severity. These include:
- general immunosuppressants: cyclophosphamide, methotrexate, or azathioprine, depending on the phase of treatment and symptom severity
- prednisone or other corticosteroids: a class of potent immunosuppressive therapies commonly used for induction, but that can cause serious side effects long-term
- Nucala (mepolizumab) or Fasenra (benralizumab): under-the-skin (subcutaneous) therapies approved for EGPA that may be used during induction or maintenance
- rituximab: an into-the-vein (intravenous) therapy approved for MPA and GPA that’s commonly used for induction and maintenance
- Tavneos (avacopan): an oral therapy approved for MPA and GPA that’s often used to reduce the need for steroids during induction
Induction therapy is typically more aggressive, while maintenance treatment focuses on long-term disease control while minimizing side effects.
Although treatment can help many patients reach AAV remission, about 30% to 50% experience relapses, or periods of new or worsening symptoms. Promptly treating AAV relapses with a new round of induction therapy can help limit long-term damage.
Regular checkups and follow-up during treatment are critical for monitoring treatment responses and side effects.
Living with AAV
Many people living with AAV continue to receive maintenance therapy for several years during remission, although some may be able to discontinue treatment earlier.
Regular follow-up care and monitoring are essential, even for people in stable remission. Patients should always report new or worsening symptoms to their healthcare providers so any necessary treatment changes can be made before serious damage occurs.
Patients may also need to adjust their usual routines to best manage the impact of AAV symptoms and medication side effects on daily life. Individuals should discuss with their care providers whether changes in diet, exercise regimens, or other lifestyle factors may be beneficial.
AAV patients and caregivers may benefit from mental healthcare, including counseling, therapy, or vasculitis support groups.
ANCA Vasculitis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.


