
ANCA-associated vasculitis types
 Fact-checked by
Fact-checked by There are three main types of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), a group of autoimmune conditions characterized by inflammation in the body’s small blood vessels.
Self-reactive antibodies called ANCAs usually trigger AAV autoimmune attacks by targeting proteins on neutrophils, a type of immune cell. This activates the neutrophils, causing them to attack cells lining blood vessels. ANCAs typically target one of two proteins — proteinase 3 (PR3) or myeloperoxidase (MPO).
AAV symptoms vary depending on where in the body this immune-mediated damage occurs. Each of the three main types of AAV tends to be more closely associated with specific ANCAs and symptom groups. Knowing the specific AAV type is key to developing an appropriate treatment and monitoring plan.
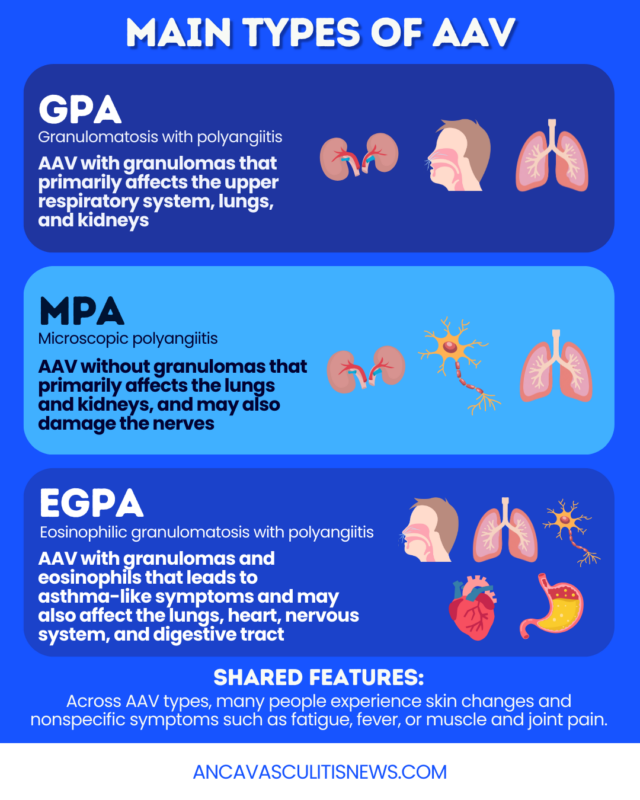
Main types of AAV
All AAV types are characterized by blood vessel inflammation (vasculitis) and tissue damage. Regardless of disease type, people living with AAV may experience nonspecific symptoms associated with this inflammation, such as:
- fever
- fatigue
- muscle and joint pain
- weight loss
The specific AAV type is classified at the time of diagnosis based on the pattern of organ involvement and certain laboratory findings. The three main AAV types include:
- granulomatosis with polyangiitis (GPA)
- microscopic polyangiitis (MPA)
- eosinophilic granulomatosis with polyangiitis (EGPA)
Each of these disease types differs in the organs most likely to be affected and the ANCAs they’re usually associated with.
Why does AAV type matter?
While these three forms of AAV share core features, AAV treatment varies by type, with EGPA generally requiring different immunosuppressant medications than MPA or GPA.
Knowing which AAV type a person also helps doctors and patients monitor the organs most likely to be affected. The specific type and pattern of organ involvement can also influence AAV prognosis.
Granulomatosis with polyangiitis (GPA)
GPA, formerly known as Wegener’s granulomatosis, is the most common type of AAV, affecting around 96.8 people per million globally. It occurs in all racial and ethnic groups, but is most common in white people. Symptoms typically emerge between the ages of 45 and 60, but may uncommonly occur in children.
GPA is commonly associated with a triad of inflammation involving the lungs, kidneys, and upper respiratory tract, which includes the nose, throat, ears, and air-filled spaces in the skull (sinuses). While they may can vary, typical symptoms of GPA may include:
- upper respiratory tract: nasal and sinus pain or congestion, nasal discharge and crusting, sores in the nose, nosebleeds, or ear infections
- lungs: cough or coughing up blood, shortness of breath, and chest pain
- kidneys: bloody or foamy urine, although kidney damage may be asymptomatic
- eyes: swelling or eye pain, vision changes
- skin: rash of purplish spots on the skin (purpura)
About 75% of people with GPA test positive for PR3-ANCAs. At the microscopic level, GPA is characterized by the formation of immune cell clumps, called granulomas, at sites of inflammation. This is a key difference between GPA and MPA, which is not characterized by granulomas. Unlike EGPA, granulomas in GPA don’t typically contain high levels of eosinophils.
Microscopic polyangiitis (MPA)
MPA is the more common form of AAV in China and Japan. It is estimated to affect around 39.2 people per million globally. It typically manifests between the ages of 50 and 60, with similar prevalence in men and women.
This form of AAV commonly affects the kidneys and lungs, although a wide range of other tissues can also be affected, including the skin and nerves outside the brain and spinal cord. Some common symptoms of MPA may include:
- kidneys: bloody or foamy urine, although it may be asymptomatic
- nervous system: tingling, weakness, or numbness
- lungs: coughing or coughing up blood, shortness of breath, chest pain
- skin: purpura
- gastrointestinal issues: stomach pain
Kidney problems occur in up to 90% of people with MPA and can progress rapidly. In some cases, severe and life-threatening kidney or lung disease is the first disease presentation.
Around 70% of MPA patients test positive for MPO-ANCAs. MPA is the only form of AAV that does not feature granulomas. Inflammation is instead more spread out, without clear masses of immune cells.
Eosinophilic granulomatosis with polyangiitis (EGPA)
EGPA, formerly called Churg-Strauss syndrome, is the least common AAV type, estimated to affect about 15.6 people per million worldwide. Although the median age at disease onset is around age 40, it can occur at any age, and affects both sexes equally.
This AAV type characteristically affects the lungs and upper respiratory system, but may eventually involve the heart, gastrointestinal tract, and nervous system. It often occurs in three stages, although this is not universal.
In the first stage, patients may experience nonspecific symptoms common to all AAV types, alongside:
- severe and poorly controlled asthma, including coughing, wheezing, and shortness of breath
- allergies, with sneezing, nasal itching, and congestion
- chronic sinus inflammation and pressure
- noncancerous growths inside the nose
As the disease progresses to stage two, immune cells called eosinophils start to invade the body’s tissues, driving:
- chest pain and difficulty breathing
- heart palpitations
- skin rashes or lesions
- stomach pain or diarrhea
Stage three can involve signs of more profound organ damage, like:
- signs of internal bleeding, including blood in stool or coughing up blood
- numbness, tingling, or nerve pain
- signs of heart disease, including irregular heartbeat, faintness, or swelling
Around 60% of adults with EGPA test negative for the common ANCA types. Similar to GPA, granulomas form in EGPA, but EGPA’s unique clinical course is driven by high levels of eosinophils. This is one way doctors can distinguish EGPA versus GPA.
How the types of AAV compare
Overall, the key features doctors use to compare the three AAV types include:
- ANCAs: PR3-ANCAs are most often linked to GPA and MPO-ANCAs to MPA, while more cases of EGPA are ANCA-negative
- granulomas: form in GPA and EGPA, but not in MPA
- eosinophils: elevated in EGPA, but not in GPA or MPA
- organ involvement: severe allergy and asthma symptoms are highly suggestive of EGPA, while MPA rarely involves the upper respiratory tract; significant kidney involvement is more common in MPA and GPA than in EGPA
Despite these differences, the types of AAV can overlap substantially, which is why classifying GPA versus MPA versus EGPA can take some time. After AAV is diagnosed, doctors will use various tests, including ANCA blood tests, tissue biopsies, and imaging studies, to evaluate these features and determine which type of the disease is present.
More recently, scientists have advocated for a new AAV classification system that relies less on these three distinct clinical subtypes and more on the specific ANCA type that’s present, although this is not yet widely used in clinical practice.
There are also several different types of vasculitis, or diseases that cause blood vessel inflammation, which can overlap with GPA, MPA, and EGPA. Physicians distinguish between AAV and other types of small vessel vasculitis by examining microscopic features of the disease and determining whether ANCAs are present.
ANCA Vasculitis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.


