ANCA-associated vasculitis treatment
 Fact-checked by
Fact-checked by Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a group of autoimmune diseases characterized by small blood vessel inflammation. The goal of AAV treatment is to promote and sustain periods of low or absent inflammatory activity, known as AAV remission.
In AAV, mistaken immune attacks cause inflammation and tissue damage. AAV medications suppress this abnormal immune activity to ease symptoms and prevent serious organ damage. Prompt and appropriate treatment can improve the long-term prognosis and quality of life for people living with AAV.
How a treatment plan is decided
Many factors can affect how AAV is treated in a specific case, including:
- Disease type: Different disease types affect different organs and can take distinct courses. Treatment strategies for microscopic polyangiitis (MPA) and granulomatosis with polyangiitis (GPA) are largely similar, but differ somewhat for eosinophilic granulomatosis with polyangiitis (EGPA).
- Disease activity: Treatment differs depending on whether AAV is active — that is, when there are new, worsening, or ongoing symptoms — or in remission, when symptoms ease or disappear. Treatment for active disease is generally more aggressive.
- Symptom severity: Symptoms can be classified as severe or nonsevere depending on whether they are likely to cause significant organ dysfunction or death. Severe AAV treatment typically requires a more aggressive approach.
- Patient-specific factors: A person’s overall health, their medication preferences, tolerance for side effects, and treatment availability can influence treatment choices.
After an AAV diagnosis, patients should work with their healthcare providers to develop a treatment plan that makes sense, considering all of these factors in their case.
Treatment phases
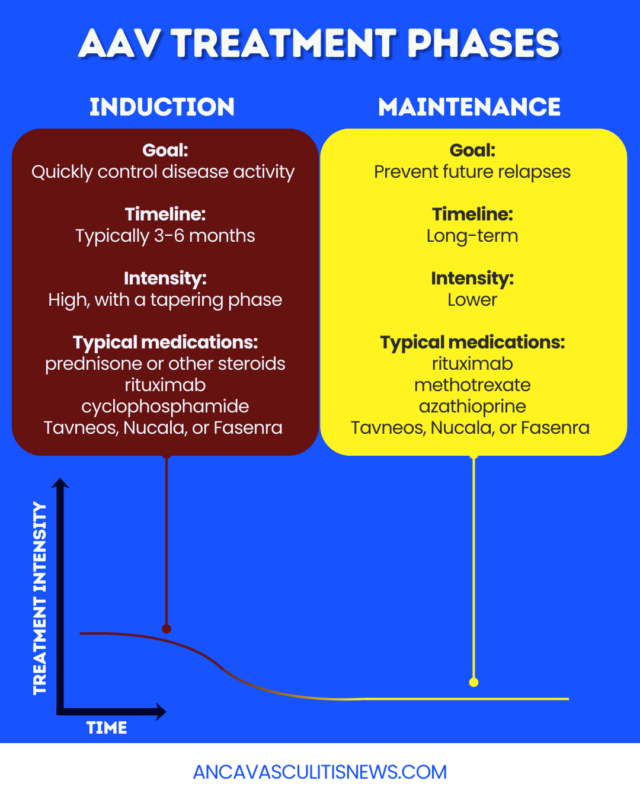
The two primary phases of AAV therapy are:
- induction: focuses on getting an active disease attack under control and pushing AAV into remission
- maintenance: aims to keep patients in remission and prevent relapses
Induction therapy for AAV typically lasts three to six months, although the duration varies. It often includes a course of corticosteroids, powerful immunosuppressants that can quickly suppress the immune system, but may have significant side effects if used long-term.
Maintenance therapy for AAV follows induction therapy. It often continues for several years, although some patients may be able to discontinue treatment earlier if their disease is well-controlled. Because this phase of treatment lasts much longer, less-aggressive treatments with fewer severe side effects are often recommended.
Medications used
Immunosuppressive medications are the cornerstone of AAV treatment guidelines. Some of these are approved for certain AAV types. Others are used off-label, meaning that they’re not specifically approved for AAV, but are given in some situations.
Targeted medications that are approved for AAV in the U.S. include:
- Fasenra (benralizumab): an under-the-skin (subcutaneous) injection therapy approved for EGPA
- Nucala (mepolizumab): a subcutaneous injection therapy approved for EGPA
- rituximab (sold as Rituxan and others): an into-the-vein (intravenous) infusion therapy approved for MPA and GPA
- Tavneos (avacopan): an oral therapy approved for MPA and GPA
Each works in a different way to suppress the abnormal immune reactions that drive AAV symptoms. Of these, all but Tavneos are a biologic therapy for AAV, meaning they’re made from components of living organisms.
Broad-acting immunosuppressants that may be used off-label for AAV include:
- azathioprine
- cyclophosphamide
- methotrexate
- mycophenolate mofetil
- prednisone or other corticosteroids (sometimes referred to as glucocorticoids or steroids)
The specific immunosuppressive drugs for AAV in each case will depend on various factors, including whether a person is in the induction or maintenance phase of treatment.
Induction therapies
For induction therapy, most patients receive prednisone plus another immunosuppressant — usually rituximab, cyclophosphamide, or methotrexate.
Corticosteroids for AAV can have significant side effects, so these medications are usually tapered off over time. Other medications may also be added to limit the need for corticosteroids, including Tavneos for MPA and GPA, and Fasenra or Nucala for EGPA.
Maintenance therapies
Long-term treatment for AAV varies depending on the specific symptom profile and estimated risk of relapse, but often involves rituximab, methotrexate, or azathioprine.
Nucala or Fasenra are recommended to maintain remission in people with EGPA, and Tavneos may be used for MPA or GPA.
Treating severe or organ-threatening disease
For severe disease activity that could be life-threatening or permanently reduce organ function, a more aggressive treatment approach is sometimes used, including a high-dose steroid regimen along with other immunosuppressants. These medications may be infused into the bloodstream in a hospital.
Other treatments that may be added include:
- intravenous immunoglobulin: involves infusing antibodies from healthy donors into the bloodstream to help normalize immune activity. It may be used for people with severe or difficult-to-treat symptoms, as well as for those who cannot tolerate or experience frequent infections from standard immunosuppressants.
- plasma exchange therapy: a blood filtering procedure that helps remove disease-driving antibodies from the blood. This may be added to the induction regimen if there is a high risk of kidney failure.
For people who are in stable remission but have end-stage kidney disease, a kidney transplant may be considered. Serious problems in the nose, sinuses, or airways may require surgery if immunosuppressant treatments and supportive care are insufficient.
Managing side effects and treatment risks
The immunosuppressive treatments used for managing AAV can come with several side effects and risks, including:
- higher chances of infections
- lower vaccine efficacy
- impaired fertility or safety concerns during pregnancy
Patients may receive preventive antibiotics or other medications to help reduce infection risk with immunosuppressants. A healthcare provider will also advise patients on when to receive specific vaccines.
People who are pregnant or considering becoming pregnant should discuss treatment options with their care providers.
Steroid medications in particular can lead to a wide range of other side effects, including bone density loss, weight gain, and mood changes. Doctors typically try to limit these risks by minimizing the dose and duration of steroid treatment.
Patients will be closely monitored for any potential side effects of AAV treatment, with the regimen adjusted as necessary if they occur.
Monitoring treatment response
It is recommended that patients maintain a regular follow-up schedule to monitor treatment efficacy and disease activity.
A key way to track if treatment is working is to monitor for any new or worsening symptoms. Doctors will likely also run blood tests to assess levels of disease-driving antibodies and other markers of immune activity, which can provide information on how well treatment is working to suppress the immune system and lower relapse risk.
Imaging tests and biopsies may sometimes be recommended to help track inflammation and damage in specific organs.
Relapse and retreatment
Even with maintenance therapies, about 30% to 50% of people with AAV experience relapses. During these periods of new or worsening symptoms, patients will need to enter a new phase of induction therapy, which may include previously used or new medications. AAV relapse treatment can also involve adjusting the maintenance regimen.
Patients should report to their doctors any noticeable changes in symptoms, as these may indicate new disease activity that requires treatment modifications.
ANCA Vasculitis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.